

ERCP Patients:
Common occurrence on 6RC, MICU, H/O
On the day/night of admission you should figure out which ERCP staff is on call currently or who will be on in the morning. IF the patient does not need to be seen until the next morning you need to page/email the on call person for the next day not overnight.
-
Dr Silverman prefers text/email communication, but is also available by pager. Likes to use FaceTime to teach
-
Dr. Johlin prefers paging (but only has a numeric pager). He does not check his email
-
Dr. Sahar perfers phone contact
Do NOT assume the ED has already talk to the ERCP provider. Always contact them in the morning or overnight in some form.
If they has been seen by Silverman, Johlin, or Sahar before, then contact that person rather than the on-call person.
Often I send an email to Dr. Silverman at night, but page/text during day. An ICU patient may require calling them at night, depending on acuity.
Labs:
-
CBC, CMP, amylase, lipase, PT/INR (Stat 5AM)
-
Blood cultures ( on admission)
Management:
-
ABX: cefoxitin/ceotetan for most. Antimicrobial guide says ceftriaxone and metronidazole. Zosyn is for those that are very sick or unstable
-
No PPX anticoagulation. No heparin or enoxaparin. If INR elevated – consider vitamin K
-
IMAGING! (load and interpret outside images)
-
Keep NPO. Can run fluids, but have stop time!
Key to these patients is all about trending labs, starting abx with any suspicion of obstruction (Transaminases are most sensitive lab, least specific) and having them ready for a procedure if necessary! And do not be afraid to contact the ERCP team for any patient you are worried about.
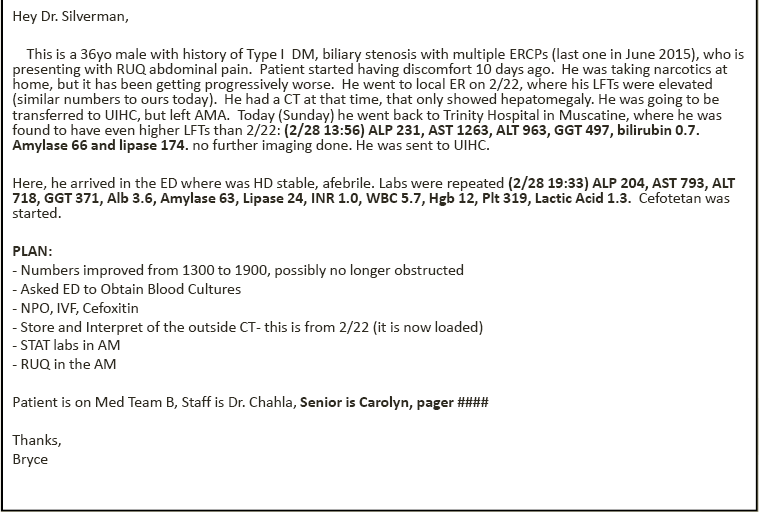
EXAMPLE EMAIL: Be sure to encrypt and use university email due to PHI
Clinical Pearls:
-
Ninety percent of cases of acute cholecystitis occur in the setting of obstruction of the cystic duct by gallstones or biliary sludge.
-
Ultrasound will show you gallstones and can show cystic ductal dilation. MRI / MRCP will show you parenchyma and ducts, better at visualizing common bile duct stone. If concerned about a perforation, order a non-contrast CT scan, x-ray is not sensitive enough due.
-
For any concerns for perforation, order stat CT, start gram negative and fungal coverage (fluconazole for candida), make patient NPO, reverse INR if needed, and call ERCP provider stat!
-
Cholangitis should be treated with immediate broad-spectrum antimicrobial therapy and, if rapid improvement is not seen, urgent endoscopic stone removal with endoscopic retrograde cholangiopancreatography.
-
ERCP compliations PPPBIC
-
Pain
-
Perforation
-
Pancreatitis
-
Bleeding
-
Infection
-
Cardiopulmonary – transient gram negative bacteremia
-
Post by Roger D. Struble Jr. MD, MPH