
Lecture by Dr. Suneja Jul 2nd 2020

Learning Objectives
OVERVIEW
Sudden loss of kidney function over hours to days
Reflected by rise in creatinine and/or decrease in urine output
-
Acute kidney injury occurs in approximately 5% to 7% of hospital admissions and up to 30% of ICU admissions.
-
Kidney Disease Improving Global Outcomes acute kidney injury (AKI) consensus guidelines define AKI as an increase in serum creatinine ≥0.3 mg/dL (26.5 µmol/L) within 48 hours, ≥1.5 times baseline (known to have occurred within the previous 7 days), or urine volume <0.5 mL/kg/h for 6 hours.
-
In patients with oliguria, the fractional excretion of sodium (FENa) can help differentiate between prerenal acute kidney injury (AKI) and acute tubular necrosis (ATN); FENa <1% indicates prerenal AKI, whereas FENa >2% indicates ATN.
-
In the setting of diuretics, a fractional excretion of urea (FEUrea) <35% can be used to diagnose prerenal acute kidney injury.
-
Kidney ultrasonography or bedside POCUS should be performed to rule out obstructive uropathy as the cause of acute kidney injury.
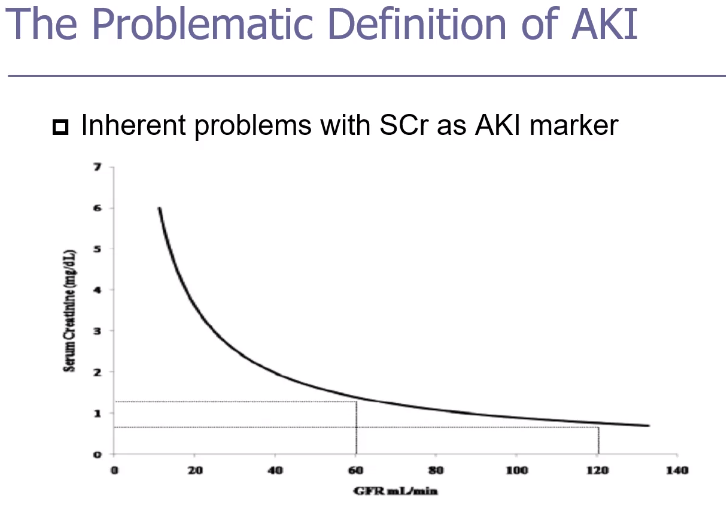
Changes in S. Cr may lag changes in GRF and may be a very late indicator of renal injury
Does not differentiate cause of renal insult
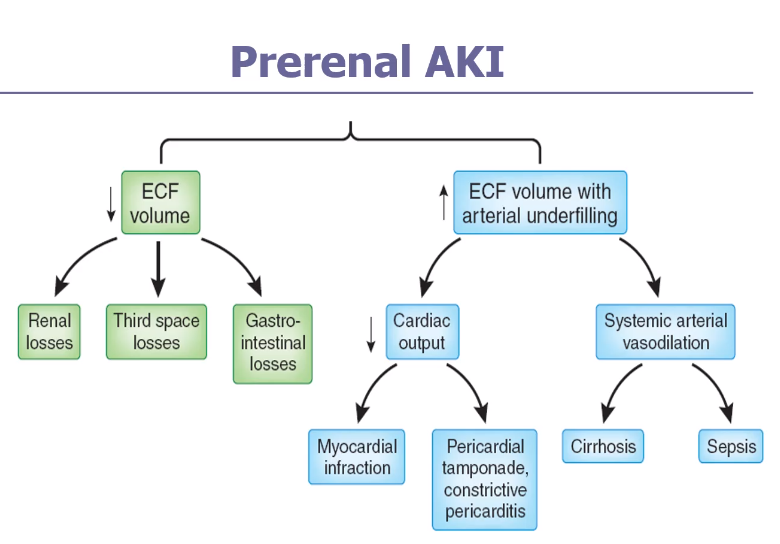
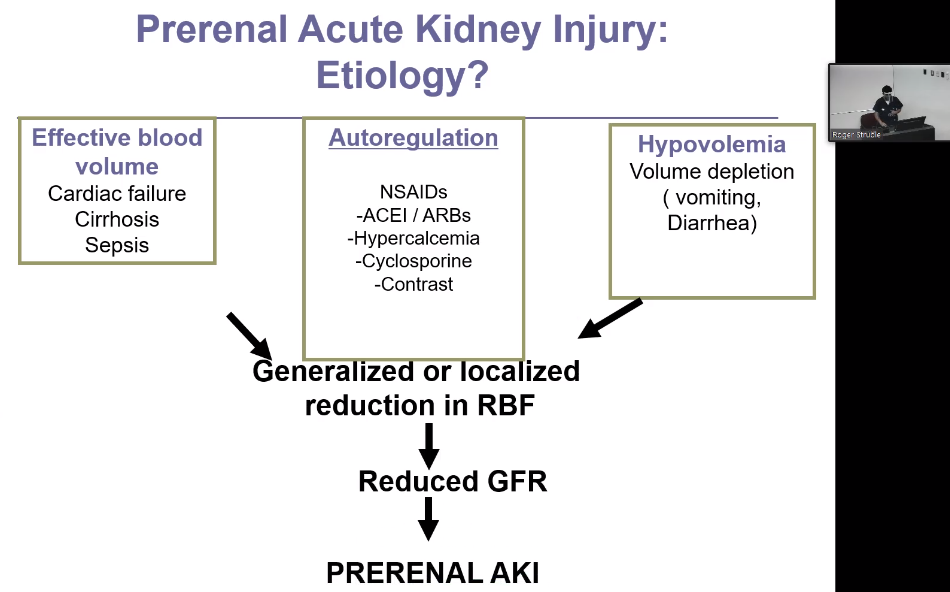
PRERENAL
Management of prerenal acute kidney injury includes discontinuation of nephrotoxins and treatment of the underlying cause.
INTRINSIC RENAL DISEASE
-
Drug-induced acute interstitial nephritis is characterized by a slowly increasing serum creatinine 7 to 10 days after exposure and should be considered in any patient with unexplained acute kidney injury who has been exposed to a potentially offending drug.
-
Large- and small-vessel causes of intrinsic acute kidney injury include bilateral renal artery obstruction, bilateral renal vein thrombosis, thrombotic microangiopathy, and atheroembolic disease.
-
Intratubular obstruction from precipitated monoclonal light chains, uric acid from tumor lysis syndrome, calcium oxalate deposition from ethylene glycol, and drugs can cause acute kidney injury.
POSTRENAL
Kidney ultrasonography is the modality of choice for diagnosing upper tract obstruction in patients with postrenal acute kidney injury.
ABDOMINAL COMPARTMENT SYNDROME
-
Strategies to minimize the development of contrast-induced nephropathy include intravenous volume expansion with isotonic fluids, use of low- or iso-osmolal contrast media, minimization of contrast volume, and discontinuation of potentially nephrotoxic medications.
-
Tumor lysis syndrome is characterized by the massive release of uric acid, potassium, and phosphate into the blood from rapid lysis of malignant cells; management of patients at high or intermediate risk includes aggressive volume expansion, management of hyperkalemia, and preventive therapy for hyperuricemia.
-
Abdominal compartment syndrome is defined as sustained intra-abdominal hypertension >20 mm Hg associated with new organ dysfunction; oliguric acute kidney injury develops from renal vein and artery compression in this setting.
MANAGEMENT
AKI: -Correction of volume / Optimization of cardiac function
-Discontinuation of antagonizing medications
-
NSAIDS / ACE inhibitors / Diuretics (if hypovolemic)
-
Avoid aminoglycosides, amphotericin, radiocontrast media
Indications for dialysis include hyperkalemia, metabolic acidosis, and pulmonary edema refractory to medical therapy; uremic symptoms; uremic pericarditis; and certain drug intoxications.
Post created by Roger Struble MD